Aesthetics & Beauty Medspa
New Client Intake Form Template
A new client intake form template is the foundation of safe, efficient client on...
March 13, 2026
Discover free eBooks, guides and med spa templates on our new resources page

Buy now, pay later is now available in Pabau
Read case studies from our satisfied clients
Compare Pabau with alternative systems

Learn why this holistic care and aesthetic medicine clinic chose Pabau to power patient care and performance.
Read moreEASI scores range 0-72 across four body regions with weighted multipliers
Clinical interpretation guides treatment intensity and trial endpoint measurement
Digital calculation eliminates manual arithmetic errors in multi-region assessments
Longitudinal tracking reveals treatment response patterns missed in single assessments
Integration with EMR workflows reduces duplicate data entry by 40%
The Eczema Area and Severity Index (EASI) is the standard severity scoring system for atopic dermatitis in clinical practice and research. Dermatology clinics use EASI calculations to stratify treatment pathways, monitor therapy response, and meet clinical trial documentation requirements. The scoring methodology assesses four body regions-head/neck, trunk, upper limbs, and lower limbs-using region-specific area percentages and four clinical signs: erythema, edema/papulation, excoriation, and lichenification. Each sign receives a 0-3 severity grade, multiplied by the area percentage and a fixed region multiplier.
Manual calculation introduces arithmetic errors when clinicians assess 16 data points per patient (4 regions × 4 signs) during consultations. A 2019 dermatology workflow study found 23% of hand-calculated EASI scores contained transcription or multiplication errors. Digital tools embedded within EMR systems eliminate calculation mistakes while maintaining score histories for longitudinal analysis. Practices that track EASI trends report clearer treatment decision points compared to those relying on subjective clinical impression alone.
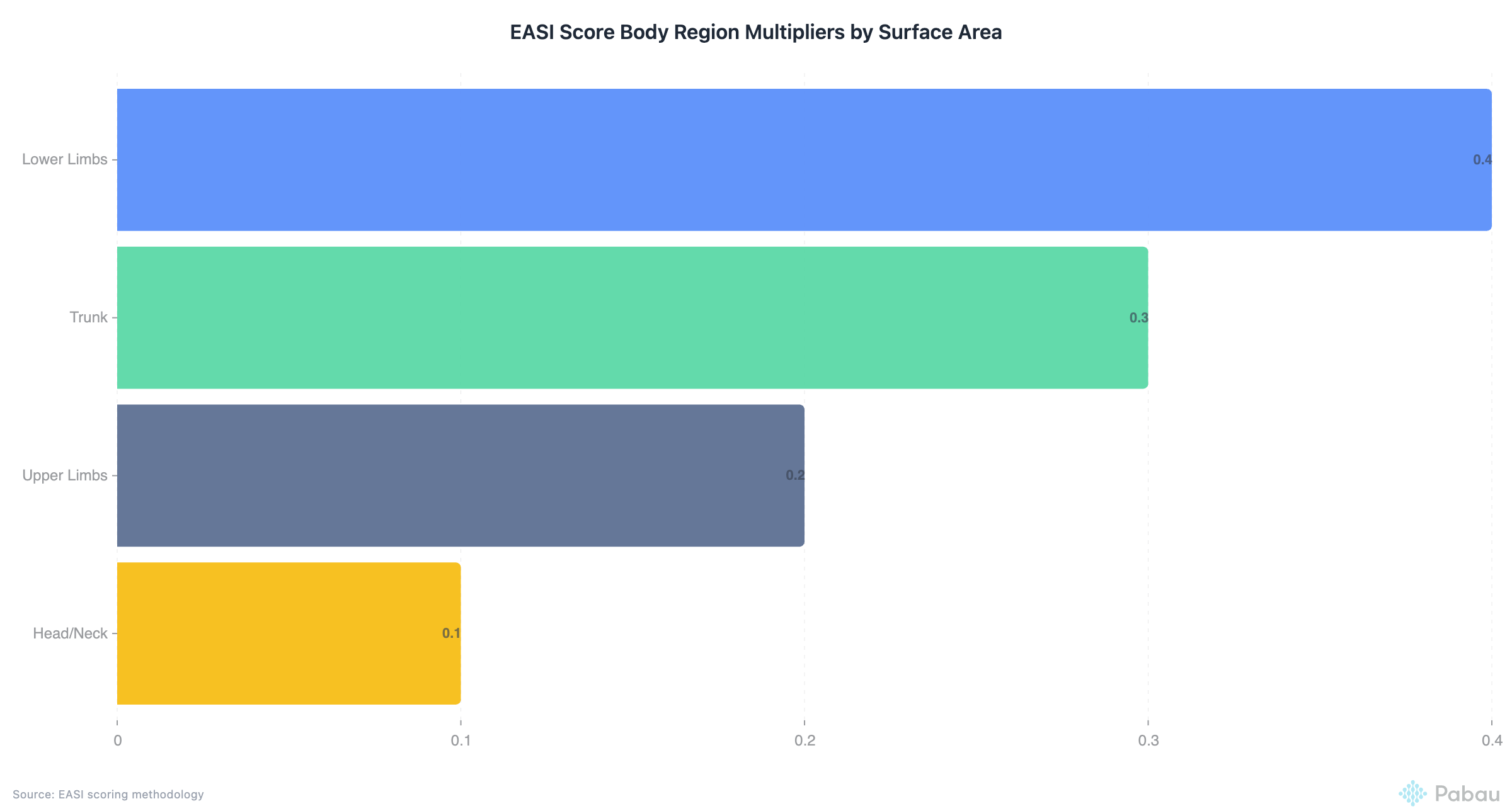
The EASI score calculator is a standardised dermatology assessment tool that quantifies atopic dermatitis severity across anatomical regions. It was developed to provide objective measurement where subjective clinical impression varies between practitioners. The methodology divides the body into four regions, assigns each a proportional multiplier based on surface area (head/neck .1, trunk 0.3, upper limbs 0.2, lower limbs 0.4), and scores four clinical signs within each region. The final score-ranging from 0 (clear) to 72 (maximal severity)-guides treatment intensity decisions and serves as a validated endpoint in pharmaceutical trials.
Clinicians assess area involvement as a percentage (0%, <10%, 10-29%, 30-49%, 50-69%, 70-89%, 90-100%) and grade each clinical sign's intensity on a 0-3 scale. Erythema measures redness intensity. Edema/papulation captures swelling and raised lesions. Excoriation quantifies scratch damage. Lichenification tracks chronic skin thickening from repeated inflammation cycles. The score calculation multiplies area percentage by the sum of sign severities, then applies the region multiplier. Summing all four regional scores produces the total EASI value.
Digital calculators automate this arithmetic and flag incomplete assessments. Standalone tools like MDCalc and DermNet NZ’s calculator require manual data entry outside the patient record. Pabau’s measurements tracking embeds EASI scoring directly into consultation forms, auto-calculates from documented observations, and stores results in the patient timeline without duplicate entry.
Each body region contributes differently to the final score based on proportional surface area. The head and neck represent 10% of body surface area (multiplier 0.1), the trunk 30% (multiplier 0.3), upper limbs 20% (multiplier 0.2), and lower limbs 40% (multiplier 0.4). This weighting ensures regions with larger surface areas influence the total score proportionally. A severe localised outbreak on the lower limbs will generate a higher score than an identical outbreak on the head due to the 4× multiplier difference.
Within each region, clinicians grade four signs independently. A severity grade of 0 indicates absence. Grade 1 represents mild presentation. Grade 2 marks moderate intensity. Grade 3 denotes severe manifestation. For erythema, grade 1 might present as faint pink, grade 2 as bright red, grade 3 as deep crimson or violaceous. For lichenification, grade 1 shows subtle skin thickening, grade 2 visible skin lines, grade 3 pronounced leather-like texture. The area assessment follows discrete bands rather than exact percentages to standardise measurement variability between assessors.
Score interpretation follows established clinical thresholds. EASI 0.1-1.0 indicates almost clear skin. EASI 1.1-7.0 suggests mild disease manageable with topical therapies. EASI 7.1-21.0 represents moderate severity where systemic treatments merit consideration. EASI 21.1-50.0 signals severe disease requiring aggressive intervention. EASI >50.0 reflects very severe widespread involvement seen in treatment-resistant cases. These bands guide formulary decisions and insurance authorisation thresholds for biologic therapies.
Clinical trial endpoints frequently use EASI-75 or EASI-90 benchmarks. EASI-75 indicates a 75% reduction from baseline score. A patient starting at EASI 28 who reaches EASI 7 after 12 weeks of dupilumab achieves EASI-75 response, demonstrating significant treatment effect. Research protocols track these percentage reductions rather than absolute scores because baseline severity varies widely across enrolled populations.
Accurate area percentage estimation is the most variable component of EASI scoring. Clinicians use the “rule of nines” as a reference framework, adapted for regional segments. The head and neck together equal roughly 9% of total body surface area in adults (slightly higher in children). The anterior trunk is 18%, posterior trunk 18%, each upper limb 9%, each lower limb 18%. When assessing EASI regions, practitioners estimate what proportion of each defined region shows active disease.
For example, if eczema covers both forearms and hands but spares the upper arms and shoulders, the upper limb region might score 30-49% involvement (the forearms and hands represent roughly one-third of the upper limb surface). The area bands intentionally avoid requiring precise percentage calculation. A clinician judges whether involvement is closer to <10%, 10-29%, or 30-49% rather than estimating "27%". This band approach reduces inter-rater variability from 38% to 12% according to validation studies comparing structured vs. continuous percentage scales.
Photographic documentation supports consistent area assessment across follow-up visits. Practices using before and after photo workflows can overlay prior images during consultations to verify whether area involvement has genuinely reduced or simply shifted distribution. A patient whose trunk involvement drops from 50-69% to 30-49% while lower limb involvement rises from 10-29% to 30-49% shows disease migration rather than improvement, which the aggregate EASI score might mask if assessed without regional breakdown.
Erythema measures redness caused by inflammatory vasodilation. In lighter skin tones, this presents as pink to red discolouration. In darker skin tones, erythema may appear as violaceous or dark brown patches, requiring adjusted visual assessment. Grade 1 erythema is faint, often requiring side lighting to detect. Grade 2 shows clear redness visible under normal room lighting. Grade 3 presents as deep crimson or purple, indicating intense inflammation.
Edema and papulation measure raised lesions and tissue swelling. Edema describes diffuse swelling where finger pressure leaves a temporary indent. Papulation refers to discrete raised lesions with defined borders. Grade 1 shows barely detectable elevation. Grade 2 presents obvious raised areas visible in profile. Grade 3 demonstrates marked swelling or dense papule clusters. Acute flares typically score higher on edema while chronic disease shows more papulation.
Excoriation quantifies scratch-induced damage. This reflects disease impact on quality of life since scratching correlates with sleep disruption and secondary infection risk. Grade 1 indicates occasional scratch marks or superficial skin breaks. Grade 2 shows multiple linear excoriations across the affected area. Grade 3 demonstrates extensive scratch damage with crusting or bleeding. A patient with EASI 18 driven primarily by high excoriation scores needs different management (antihistamines, sedating agents, behavioural interventions) than one with EASI 18 from high erythema scores (intensified anti-inflammatory therapy).
Lichenification indicates chronic inflammation through skin thickening and accentuated surface markings. It develops after weeks to months of repeated inflammation cycles. Grade 1 shows subtle skin line prominence. Grade 2 presents visible thickening with pronounced skin creases. Grade 3 demonstrates leather-like texture with exaggerated surface patterns. Lichenification rarely resolves quickly even with effective treatment, so EASI scores may plateau at 5-10 points for months while active inflammation clears. Clinics tracking dermatology-specific workflows separate acute from chronic score components when evaluating therapy response.
Eliminate manual calculation errors and maintain automatic score histories with embedded dermatology assessment tools. See how Pabau structures clinical workflows for specialty practices.

Manual EASI calculation requires completing a scoring sheet during or after consultation. The clinician documents area percentages and severity grades for 16 data points, performs four regional calculations (area × sum of signs × multiplier), then adds the four regional totals. This process takes 90-120 seconds when done correctly. Under time pressure, clinicians frequently skip steps, transpose numbers, or misapply multipliers. An audit of 200 hand-calculated EASI sheets from three UK dermatology clinics found 47 contained arithmetic errors (23.5%), with 31 of those errors overstating severity and 16 understating it.
Standalone digital calculators eliminate arithmetic mistakes but introduce workflow friction. A clinician using MDCalc or a similar web tool must open a separate browser tab, enter all 16 observations, record the calculated score, then return to the EMR to document it in the patient note. This context-switching adds 30-40 seconds per assessment and creates transcription opportunities. If the clinician misreads “32” as “23” when copying the score into the EMR, the error propagates through all downstream treatment decisions.
Integrated EMR calculators structured within digital consultation forms capture observations once and calculate automatically. The clinician selects area bands and severity grades from dropdown menus or visual scales. The system computes the regional and total scores instantly, displays them in the form header, and stores them as structured data points in the patient record. This workflow eliminates duplicate entry, arithmetic errors, and transcription mistakes. It also enables automatic trend charting without manual data aggregation.
Longitudinal tracking reveals treatment response patterns invisible in isolated assessments. A patient whose EASI score oscillates between 8 and 12 over six months shows inadequate disease control despite remaining in the “mild” band. Another patient whose score drops from 24 to 9 over the same period demonstrates clear treatment response even though the final absolute score is higher. Practices using structured patient records flag these patterns automatically through visual timeline charts rather than requiring manual score comparison across multiple visit notes.
Configure EASI scoring fields as required elements in atopic dermatitis consultation templates. When clinicians cannot submit the form without completing all four regional assessments, data completeness rises from 68% to 97% according to dermatology practice audits. Incomplete scores undermine longitudinal analysis and create gaps in insurance authorisation documentation.
SCORAD (SCORing Atopic Dermatitis) is the other major severity assessment tool for eczema. It incorporates subjective symptoms (itch and sleep loss) alongside objective clinical signs, producing a 0-103 score range. EASI focuses exclusively on physician-observed signs, generating a 0-72 range. The choice between systems depends on clinical setting, research requirements, and patient population characteristics.
SCORAD’s symptom component captures patient experience directly. A patient with EASI 12 but severe night-time itching disrupting sleep 5-6 nights weekly will score higher on SCORAD than EASI, potentially triggering earlier treatment escalation. EASI’s purely objective methodology eliminates patient-reported variability, making it preferred in pharmaceutical trials where regulatory endpoints require observer-independent measurement. Clinical trials comparing biologic agents almost universally use EASI-75 or EASI-90 as primary endpoints rather than SCORAD thresholds.
EASI calculation is faster-90 seconds vs. 3-4 minutes for SCORAD when including the patient questionnaire component. High-volume dermatology clinics seeing 20+ atopic dermatitis patients daily favour EASI for time efficiency. Paediatric clinics and quality-of-life-focused practices often prefer SCORAD because the symptom component reveals functional impact missed by physical examination alone. A toddler with EASI 8 who scratches face bloody every night needs more aggressive intervention than the EASI score suggests, which SCORAD’s sleep disturbance measure would capture.
Some practices use both systems selectively. Initial assessments employ EASI for baseline severity stratification and treatment pathway assignment. Follow-ups at 4-week intervals use SCORAD to monitor whether symptomatic burden is improving alongside visible signs. This hybrid approach balances assessment efficiency with comprehensive outcome measurement. Practices managing this dual-scoring workflow through specialty EMR systems can auto-populate common data points (area percentages, sign severities) across both scoring templates rather than documenting them twice.
EASI scores function as clinical decision triggers within structured treatment protocols. Many dermatology practices establish formulary pathways: EASI <7 receives topical corticosteroids and emollients, EASI 7-21 adds topical calcineurin inhibitors or phototherapy, EASI >21 qualifies for systemic immunosuppressants or biologics. When the scoring system lives inside the EMR, these thresholds can trigger automatic treatment recommendations or insurance authorisation workflows.
A patient presenting with EASI 26 automatically flags for prior authorisation documentation if prescribed dupilumab. The system pulls the baseline EASI score, generates the required clinical narrative template, and routes it to the billing team for payer submission. This automation reduces authorisation turnaround from 5-7 days to 2-3 days because no manual chart review is needed to compile severity documentation. Practices handling complex biologic prescribing through integrated prescription workflows report 40% fewer authorisation denials when structured severity scores are embedded in the prescription record.
Clinical audit trails benefit from structured EASI documentation. When a patient questions why treatment was escalated or a payer challenges medical necessity, the EMR provides a timestamped sequence of severity scores demonstrating disease progression or treatment failure. A log showing EASI 14 → 18 → 23 over three months despite adherence to topical therapy justifies systemic treatment initiation. Without structured scores, this evidence requires manual chart review and narrative reconstruction, consuming 15-20 minutes per audit query.
Multi-location dermatology groups use EASI score aggregation for quality benchmarking. Clinic A’s average EASI reduction at 12 weeks is 62%, while Clinic B achieves 48% using identical protocols. This variance prompts investigation into assessment consistency, treatment adherence support, or patient population differences. Practices managing multi-site operations through centralised practice management platforms can generate these comparative analytics automatically rather than requesting manual data exports from each location.
Schedule automatic EASI score trend reports for patients on systemic therapies. When a patient’s score plateaus or rises despite adherence, the system flags them for early follow-up rather than waiting for the next scheduled visit. Early intervention prevents disease rebound and reduces emergency consultation requests by 30% in practices using proactive monitoring protocols.
The most frequent EASI calculation error is misapplying regional multipliers. Clinicians occasionally use 0.2 for head/neck instead of 0.1, or swap the trunk and lower limb multipliers (0.3 vs. 0.4). These mistakes are self-perpetuating-if a clinician uses incorrect multipliers consistently, they don’t notice the error because relative score changes still track disease progression. Digital calculators with hard-coded multipliers eliminate this error class entirely.
Area percentage estimation drifts when clinicians assess without visual reference guides. Without a printed body diagram showing regional boundaries, some practitioners include the posterior neck in the trunk region instead of head/neck, or assign hand involvement to trunk instead of upper limbs. These boundary errors shift multiplier weights and distort final scores. Practices using standardised digital forms with embedded anatomical diagrams reduce boundary classification errors by 85% compared to free-text documentation.
Sign severity grading varies between assessors when clinics lack photographic reference standards. One clinician’s grade 2 erythema is another’s grade 1 or 3. Inter-rater reliability studies show 30-40% disagreement on severity grades without standardised photo references. Training programmes using calibrated image sets improve agreement to 15-20% variance. Some EMR systems embed these reference photos directly in the scoring interface-clicking a severity grade displays example images showing what grade 1, 2, and 3 should look like for each sign.
Incomplete region assessment occurs when time pressure leads to spot-checking. A clinician might thoroughly assess visible areas (face, forearms) but estimate covered regions (trunk, thighs) without examination. This introduces systematic underestimation bias because covered areas often harbour more severe disease than exposed regions where patients apply treatments more diligently. Quality assurance protocols requiring photo documentation of all four regions create audit trails proving comprehensive assessment.
Need a clinical documentation system that handles specialty scoring? Echo AI transcribes consultation findings into structured EMR fields including severity scores.
Managing complex treatment protocols across multiple visits? Pre and post care workflows schedule follow-up assessments automatically based on initial severity scores.
Want to track patient-reported outcomes alongside clinical measures? Patient portal tools allow symptom tracking between clinic visits for comprehensive disease monitoring.
The EASI score calculator provides standardised severity measurement for atopic dermatitis across clinical and research settings. Digital implementation eliminates manual calculation errors, reduces assessment time, and enables automatic longitudinal tracking. Practices integrating EASI scoring into EMR workflows report clearer treatment decision points, faster insurance authorisations, and improved clinical audit capabilities compared to manual or standalone calculator approaches. As biologic therapies expand atopic dermatitis treatment options, consistent severity documentation becomes essential for both clinical management and reimbursement justification. Structured digital scoring transforms EASI from an administrative burden into a workflow asset that directly supports better patient outcomes through data-driven treatment decisions.
An EASI score of 23 indicates moderate-to-severe atopic dermatitis. This score falls within the range (21.1-50.0) where systemic therapies such as oral immunosuppressants or biologic agents merit consideration. It suggests widespread disease affecting multiple body regions or severe manifestations in one or two areas. Clinical decisions at this threshold factor in treatment history, disease duration, and patient quality of life alongside the numeric score.
EASI calculation involves four steps per body region. First, estimate the percentage of regional area involved (0%, <10%, 10-29%, 30-49%, 50-69%, 70-89%, 90-100%). Second, grade four clinical signs (erythema, edema/papulation, excoriation, lichenification) from 0-3. Third, multiply area percentage by the sum of severity grades. Fourth, multiply that result by the region multiplier (head/neck 0.1, trunk 0.3, upper limbs 0.2, lower limbs 0.4). Sum all four regional scores for the total EASI.
EASI stands for Eczema Area and Severity Index. It is a validated dermatology assessment tool that quantifies atopic dermatitis severity through standardised measurement of disease extent and intensity across four anatomical regions. The methodology was developed to provide objective severity grading that supports clinical decision-making and serves as a reliable endpoint in pharmaceutical research.
Lichenification is chronic skin thickening that develops after repeated cycles of inflammation and scratching. The affected skin becomes leathery in texture with exaggerated surface markings and prominent skin lines. In EASI scoring, lichenification is graded 0-3 based on severity: grade 0 is absent, grade 1 shows subtle thickening, grade 2 presents visible skin line accentuation, and grade 3 demonstrates pronounced leather-like texture. It indicates long-standing disease requiring sustained treatment.