Mental Health & Therapy Therapy & Counseling
Cognitive Defusion
Clients often arrive in therapy locked in a struggle with their own thinking, co...
May 27, 2026

Buy now, pay later is now available in Pabau
A psychiatric evaluation template standardises the assessment process, ensuring comprehensive documentation of a patient’s mental health status, history, and treatment needs
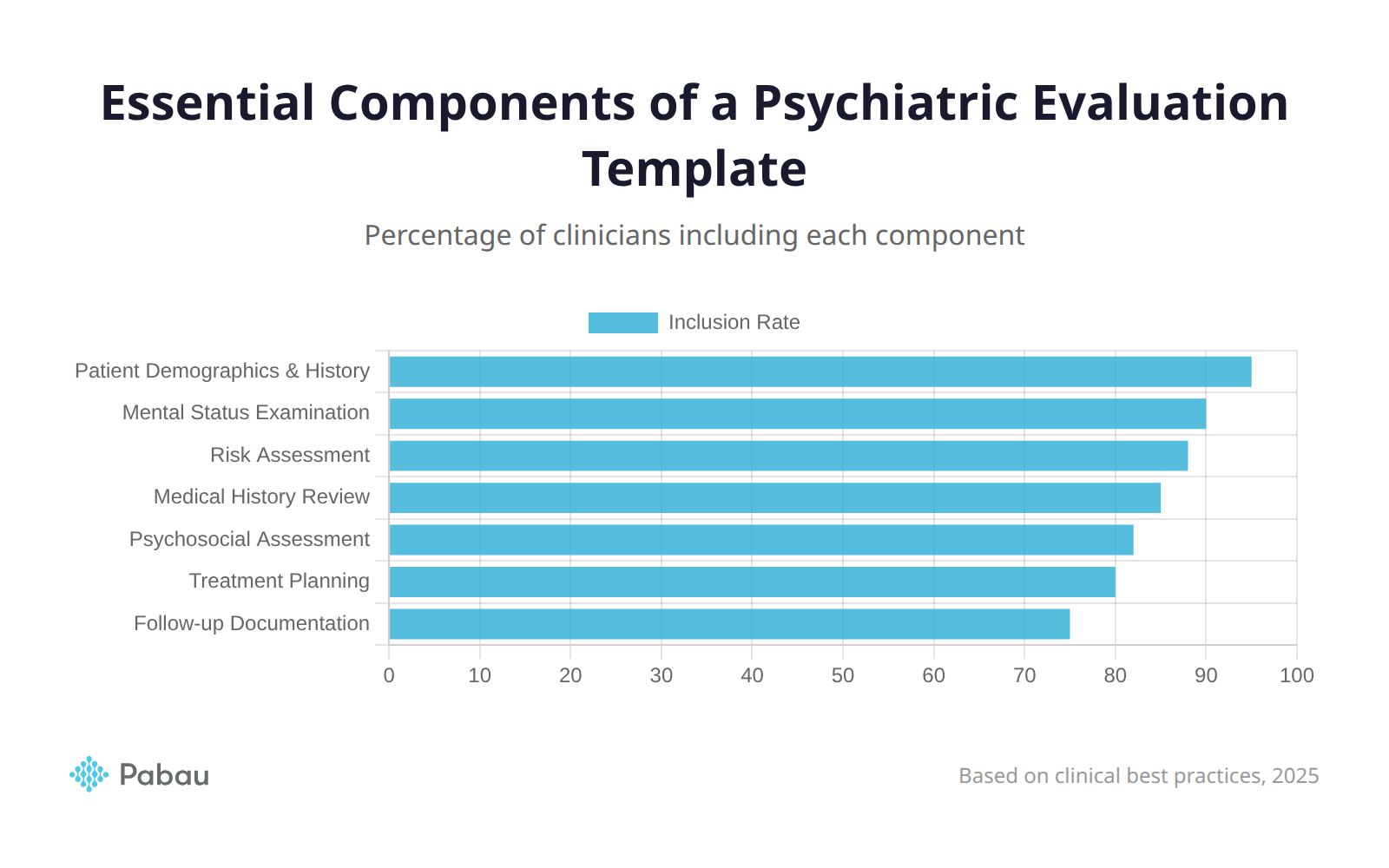
Essential template components include patient demographics, chief complaint, history of present illness, mental status examination, risk assessment, and treatment planning sections
Digital psychiatric evaluation templates integrated with EMR systems improve efficiency, reduce errors, and enhance care coordination compared to paper-based methods
Customising your psychiatric evaluation template for different patient populations and specialties ensures culturally sensitive, age-appropriate assessments
Pabau’s mental health EMR offers customisable psychiatric evaluation templates with secure storage, automated workflows, and compliance-ready documentation features
Finding yourself in need of a structured psychiatric evaluation template for your practice? Whether you’re a psychiatrist, clinical psychologist, or licensed therapist, having a comprehensive psychiatric evaluation template is essential for conducting thorough mental health assessments. This guide will walk you through every component of an effective psychiatric evaluation template, from patient intake to treatment planning, whilst showing you how digital tools can streamline your workflow.
A free, printable 8-page psychiatric evaluation form with patient information, mental status examination, risk assessment, and treatment planning sections. Print-ready PDF format.
A psychiatric evaluation is a comprehensive assessment conducted by mental health professionals to evaluate an individual’s mental health status, identify psychiatric disorders, and develop appropriate treatment plans. For example, when a patient presents with symptoms of depression or anxiety, a thorough psychiatric evaluation helps clinicians determine the underlying causes and most effective interventions.
These evaluations serve multiple purposes in clinical practice. They provide baseline data for diagnosis, establish treatment priorities, inform medication decisions, and create a roadmap for ongoing care. They also facilitate communication between healthcare providers and ensure continuity of care across different treatment settings.
In the US, psychiatric evaluations follow diagnostic criteria set out in the DSM-5-TR (Diagnostic and Statistical Manual of Mental Disorders, Text Revision, published by the American Psychiatric Association). In the UK and internationally, clinicians may also use the ICD-11 (International Classification of Diseases) published by the World Health Organisation. Many clinicians reference both systems, and your evaluation template should accommodate either.
A comprehensive psychiatric evaluation consists of several interconnected components that together create a complete picture of the patient’s mental health.
The clinical interview forms the foundation of any psychiatric evaluation. During this face-to-face conversation, clinicians gather detailed information about the patient’s current symptoms, life experiences, and overall functioning. Effective interviewing requires both clinical expertise and interpersonal skills to build rapport whilst collecting accurate information.
The mental status examination (MSE) provides a structured snapshot of the patient’s current psychological state. This systematic observation assesses appearance, behaviour, speech, mood, thought processes, and cognitive abilities. As a result, the MSE helps clinicians identify immediate concerns and track changes over time.
Psychological testing may be incorporated when additional objective data is needed. Standardised assessments like the PHQ-9 for depression or the GAD-7 for anxiety provide quantifiable measures of symptom severity. These tools help monitor treatment progress and support evidence-based decision-making.
Collateral information from family members, previous providers, or medical records often proves invaluable. This additional context helps verify patient reports, identify safety concerns, and understand how symptoms impact daily functioning.
An effective psychiatric evaluation template includes several essential sections that systematically capture all relevant clinical information. Each component serves a specific purpose in building a comprehensive assessment.
The table below provides a quick reference for the essential sections your template should include:
| Section | Purpose | Key Elements |
|---|---|---|
| Patient Demographics | Identity and administrative data | Name, DOB, gender identity, insurance, emergency contact |
| Chief Complaint | Patient’s presenting concern | Direct quote in patient’s own words |
| History of Present Illness | Symptom timeline and context | Onset, severity, triggers, functional impact, prior treatment |
| Past Psychiatric History | Previous mental health treatment | Diagnoses, hospitalisations, medication trials, therapy history |
| Medical and Family History | Physical health and genetic factors | Current conditions, medications, allergies, family psychiatric history |
| Substance Use History | Substance-related risk factors | Type, frequency, quantity, withdrawal history |
| Social History | Psychosocial context | Education, employment, housing, trauma, support systems |
| Mental Status Examination | Current psychological state | Appearance, mood/affect, thought process, cognition, risk |
| Risk Assessment | Safety evaluation | Suicidal/homicidal ideation, plan, means, protective factors |
| Diagnosis | Clinical formulation | DSM-5-TR/ICD-11 diagnoses, differentials, rule-outs |
| Treatment Plan | Recommended interventions | Medications, therapy, referrals, follow-up schedule, safety plan |
This foundational section captures basic demographic details that establish the patient’s identity and facilitate administrative processes. Include the patient’s full legal name, date of birth, current address, and contact telephone number. Additionally, record gender identity, preferred pronouns, race, and ethnicity to ensure culturally competent care.
Insurance information and policy numbers enable billing and verify coverage for recommended treatments. Documenting an emergency contact provides a safety resource should crisis situations arise during or after treatment.
The chief complaint section records the patient’s primary concern in their own words. For example, a patient might state, “I can’t sleep and feel worried all the time.” This direct quote captures their subjective experience and establishes the evaluation’s focus.
The history of present illness chronicles the timeline of current symptoms from onset to present. Start with when symptoms first appeared and how they have evolved over time. Document symptom severity, frequency, and duration. Identify any precipitating factors and previous attempts to manage symptoms.
When documenting history of present illness, use a chronological narrative that clearly connects symptom onset with life events. This temporal relationship often reveals important diagnostic clues and helps patients understand how their experiences relate to their mental health.
Understanding a patient’s historical context is crucial for accurate diagnosis and safe treatment planning. Your psychiatric evaluation template should thoroughly document both psychiatric and medical backgrounds.
This section provides essential information about previous mental health experiences. Document all prior psychiatric diagnoses, including when they were made and by whom. Record previous hospitalisations, including dates, facilities, and reasons for admission.
Detail past psychiatric treatments, including psychotherapy types and perceived effectiveness. Medication trials deserve particular attention. List all psychiatric medications previously tried, including dosages, effectiveness, and reasons for discontinuation. This information prevents repeating unsuccessful treatments.
Comprehensive medical history documentation helps identify conditions that may contribute to psychiatric symptoms or complicate treatment. List all current medical diagnoses and ongoing treatments. Document current medications, including over-the-counter supplements. Note all known allergies, particularly medication allergies.
Be aware that several medical conditions can mimic or exacerbate psychiatric symptoms. Thyroid disorders, neurological conditions, autoimmune diseases, and vitamin deficiencies should be screened for where clinically indicated. A thorough medical history helps avoid misattributing medical symptoms to a psychiatric cause.
Family psychiatric and medical history provides valuable information about genetic predispositions. Document mental health conditions in first-degree relatives, including diagnoses and treatments. Note any family history of suicide attempts, as this significantly impacts risk assessment.
Understanding a patient’s social context and daily functioning provides crucial information for treatment planning and identifying support resources.
Substance use significantly impacts psychiatric symptoms and treatment outcomes. Document current and past use of alcohol, tobacco, cannabis, and other substances. For each substance, record frequency, quantity, and date of last use. Assess for problematic use patterns or substance use disorders.
The social history section captures how patients function in their daily lives. Document educational background, current employment status, and relationship status. Describe living situation and quality of social supports. Include any history of trauma, approaching this sensitively as patients may not be ready to disclose everything initially.
The mental status examination (MSE) is a structured observation that captures the patient’s current psychological state. Including a comprehensive MSE section in your psychiatric evaluation template ensures consistent documentation of this critical assessment.
Appearance and behaviour describe how the patient presents physically. Note grooming, hygiene, and dress appropriateness. Observe behaviour during the interview: are they cooperative, guarded, or agitated? For example, “Patient appeared dishevelled with poor hygiene and displayed psychomotor retardation.”
Speech and mood assessment includes rate, volume, and tone. Is speech pressured and rapid, or slow and monotone? Mood is what the patient reports (“I feel depressed”), whilst affect is what you observe. Describe affect’s range, intensity, and appropriateness.
Thought process and content examines how patients think and what they think about. Is thought process logical, or tangential and disorganised? Screen for delusions, obsessions, and suicidal or homicidal ideation. Document the specific nature of any concerning thoughts.
Cognition and risk assessment evaluate orientation, attention, concentration, and memory. Systematically evaluate suicide risk by asking about thoughts, plans, means, and intent. Similarly, assess risks of harm to others. Document your risk assessment thoroughly and implement appropriate safety interventions.
Risk assessment is one of the most critical components of any psychiatric evaluation. Your template should include structured prompts that guide clinicians through a systematic safety evaluation.
Several validated tools support structured risk assessment:
Current best practice in risk assessment favours a formulation-based approach over simple categorical ratings (e.g. “low/moderate/high”). This means documenting specific risk factors (e.g. previous attempts, access to means, substance use, recent losses) alongside protective factors (e.g. social support, reasons for living, treatment engagement), and articulating a clinical narrative about the patient’s overall risk profile.
Your template should also prompt for assessment of harm to others, including specific questions about homicidal ideation, violent behaviour history, and access to weapons.
After gathering comprehensive information, the assessment section synthesises findings into diagnostic impressions and treatment recommendations.
List potential diagnoses using DSM-5-TR criteria (or ICD-11 for UK/international practice), prioritised from most to least likely. Explain the clinical reasoning supporting each diagnosis. For example: “Major Depressive Disorder, recurrent episode, moderate severity, supported by persistent low mood, anhedonia, and sleep disturbance for three months.”
Include a biopsychosocial formulation that integrates biological factors (genetics, medical conditions, substance use), psychological factors (coping style, personality, trauma history), and social factors (relationships, employment, housing). This formulation helps contextualise the diagnosis and informs treatment priorities.
The treatment plan translates assessment findings into concrete next steps. Recommend specific interventions, including psychotherapy type and frequency, psychiatric medications with rationale, and referrals to specialists. Include patient education about diagnoses and treatments. Document informed consent discussions about medication risks, benefits, and alternatives.
Make recommendations realistic and patient-centred. Consider the patient’s preferences, resources, and readiness to engage in treatment. Collaborative treatment planning increases adherence and outcomes.
DSM-5-TR Diagnostic Criteria: The American Psychiatric Association’s manual (Text Revision, 2022) provides standardised diagnostic criteria. Keep this accessible for diagnostic accuracy.
Standardised Assessment Tools: Incorporate validated screening instruments like the PHQ-9 and GAD-7. Track with measurements software for objective data.
Risk Assessment Protocols: Use structured tools like the C-SSRS to evaluate suicide risk. Learn more about compliant documentation practices.
APA Practice Guidelines: The APA’s Psychiatric Evaluation of Adults guideline outlines recommended assessment components and clinical decision-making frameworks.
Informed consent is a fundamental part of any psychiatric evaluation. Your template should include a section documenting that consent was obtained, what was explained to the patient, and any relevant capacity considerations.
In the United States, informed consent requirements vary by state but generally require that patients understand the purpose of the evaluation, what information will be collected, and how it will be used. Document the patient’s capacity to consent. For involuntary evaluations, document the legal basis (e.g. state civil commitment statute) and the specific criteria met.
Be aware of Tarasoff duty (duty to warn/protect) obligations, which vary by state. When a patient makes a credible threat against an identifiable third party, clinicians may have a legal duty to take protective action. Document your assessment of any such disclosures and the actions taken.
In England and Wales, the Mental Capacity Act 2005 establishes the framework for assessing whether a patient has the capacity to consent to evaluation and treatment. The Act’s five statutory principles must be followed, including the presumption of capacity and the requirement to take all practicable steps to help a patient make their own decision.
For patients under 18, Gillick competence (following the 1985 House of Lords ruling) determines whether a minor can consent to their own treatment without parental agreement. Your template should include prompts for documenting capacity assessment in minors.
Where a patient lacks capacity or is detained under the Mental Health Act 1983, document the legal framework under which the evaluation is being conducted, the section of the Act applied, and the involvement of an Approved Mental Health Professional (AMHP) where required.
Whilst core components remain consistent, effective psychiatric evaluation templates adapt to specific contexts and patient populations. Customisation ensures relevant, comprehensive assessments across diverse clinical situations.
Age-appropriate adaptations recognise that children, adults, and elderly patients require different approaches. A pediatric psychiatric evaluation template should emphasise developmental milestones, behavioural observations, parent/caregiver input, school functioning, and family dynamics. Adolescent evaluations address identity development, peer relationships, and age-specific risk factors (self-harm, substance experimentation). Geriatric assessments include cognitive screening (such as the MoCA or MMSE) and evaluation of functional independence, polypharmacy risks, and caregiver burden.
Specialty-specific modifications reflect different clinical focuses. Addiction psychiatry templates emphasise detailed substance use history. Forensic evaluations include extensive legal history. Consultation-liaison psychiatry focuses on medical-psychiatric interactions.
Cultural considerations ensure sensitivity to diverse backgrounds. Include questions about cultural identity and religious beliefs. Recognise that some cultures somatise emotional distress, whilst others may stigmatise mental health treatment. Use interpreters when needed and remain curious about cultural factors shaping the patient’s experience.
Accurate coding supports appropriate reimbursement and documentation compliance. The following CPT codes are commonly associated with psychiatric evaluations in the United States:
| CPT Code | Description | Typical Use |
|---|---|---|
| 90791 | Psychiatric diagnostic evaluation (no medical services) | Initial evaluation by a psychologist or therapist |
| 90792 | Psychiatric diagnostic evaluation with medical services | Initial evaluation by a psychiatrist or PMHNP (includes medication management) |
| 99205 | Office visit, new patient, high complexity | May be used alongside 90792 for complex initial presentations |
| 96127 | Brief emotional/behavioural assessment | Administration of standardised screening tools (PHQ-9, GAD-7) |
UK clinicians using NHS coding or private billing frameworks will reference different code sets. Your template should include a billing/coding section appropriate to your practice jurisdiction.
The choice between digital and paper psychiatric evaluation templates significantly impacts workflow efficiency and documentation quality.
Digital psychiatric evaluation templates integrated with electronic medical record (EMR) systems offer substantial advantages. Auto-population features pull existing patient information into evaluation forms, eliminating redundant data entry. Drop-down menus and checkboxes speed documentation whilst ensuring completeness.
Digital templates enable real-time collaboration between providers. Multiple team members can access evaluations simultaneously, facilitating consultation and care coordination. Integration with online forms allows patients to complete intake information before appointments, maximising face-to-face time for clinical assessment.
Compliant digital systems provide secure storage with encrypted transmission and granular access controls. In the US, this means HIPAA-compliant infrastructure with access audit trails. In the UK, systems must comply with UK GDPR and the Data Protection Act 2018, with appropriate safeguards for special category health data. Backup systems prevent data loss, and search functions enable quick retrieval of historical information.
Paper psychiatric evaluation templates still serve specific purposes despite digital advantages. A printable psychiatric evaluation template in PDF or Word format may be preferred when technology is unavailable, during system outages, or in settings where devices are restricted (e.g. inpatient units). Paper templates present challenges including storage requirements and information sharing difficulties.
When using paper templates, implement systematic scanning and digitisation processes. Store paper records securely in locked files with restricted access. Consider transitioning to electronic medical records as your practice evolves.
If transitioning from paper to digital templates, start by digitising your most commonly used evaluation forms first. This allows your team to build confidence with the new system whilst maintaining familiar workflows for complex assessments.
Modern mental health practices require efficient, secure systems that support quality care whilst reducing administrative burden. Pabau’s mental health EMR software provides comprehensive tools specifically designed for psychiatric and psychological practices.
Customisable templates form the foundation of Pabau’s evaluation capabilities. Access a library of pre-built psychiatric evaluation templates that cover all essential assessment components. Alternatively, create fully customised templates that match your specific practice needs without programming knowledge.
Digital patient intake through Pabau’s client portal allows patients to complete medical history and symptom questionnaires before their first appointment. This information automatically populates into your evaluation template, eliminating duplicate data entry and maximising clinical time.
The secure infrastructure protects sensitive mental health information with encryption, access controls, and comprehensive audit trails, supporting compliance with HIPAA (US) and UK GDPR requirements. Role-based permissions ensure that only authorised staff access patient records.
Automated workflows reduce administrative tasks and improve consistency. Set up reminders for follow-up appointments, medication reviews, or periodic reassessments. Create templates for treatment plans and progress notes that link directly to evaluation data. This integration eliminates redundant documentation and ensures care plan alignment with assessment findings.
Collaborative features facilitate team-based care. Share evaluations securely with other providers, attach records to referrals, and maintain comprehensive communication logs. This coordinated approach improves outcomes for patients with complex needs requiring multiple specialists.
Ready to transform your psychiatric evaluation process? Try Pabau free for 30 days and experience the difference integrated mental health software makes in your practice efficiency and patient care quality.
“Since implementing Pabau’s mental health EMR, our psychiatric evaluation process has become dramatically more efficient. The customisable templates ensure we capture all necessary information consistently, whilst automated workflows free our clinicians to focus on patient care rather than paperwork. Our team particularly appreciates how patient intake forms populate directly into evaluation templates – it’s saved us hours every week and improved the quality of our initial assessments.”
A comprehensive initial psychiatric evaluation typically takes 60 to 90 minutes, though complex cases may require longer. Follow-up psychiatric evaluations are usually shorter, ranging from 30 to 60 minutes. The duration depends on the complexity of the patient’s history, the number of symptoms being assessed, whether collateral information is available, and whether standardised assessment tools are administered.
A psychiatric evaluation is conducted by psychiatrists or psychiatric nurse practitioners and focuses on diagnosing mental disorders, assessing medical contributions to psychiatric symptoms, and determining medication needs. Psychological assessments are performed by psychologists and often emphasise formal psychological testing, cognitive evaluations, and personality assessments. Many patients benefit from both types of evaluation, with psychiatrists and psychologists collaborating on comprehensive care.
Whilst having a core psychiatric evaluation template provides helpful structure, best practice involves customising templates for different patient populations and clinical contexts. Children require developmental history emphasis that adults do not need. Elderly patients benefit from focused cognitive screening. Specialty evaluations for addiction or trauma need specific content areas. However, maintaining core components across all templates ensures comprehensive assessments regardless of customisation.
Completed psychiatric evaluations must be stored securely in compliance with applicable regulations. In the US, this means HIPAA-compliant electronic medical record systems with encryption, access controls, and regular backups. In the UK, systems must comply with UK GDPR and the Data Protection Act 2018. Only authorised personnel with legitimate clinical need should have access. If using paper evaluations, store them in locked filing cabinets within secure areas and maintain them for the legally required retention period (typically 7 to 10 years for adults in the US; 8 years after treatment ends for adults in the UK under NHS guidelines, or until the patient turns 25 for children).
Yes, obtaining informed consent before a psychiatric evaluation is both an ethical requirement and legal best practice. Patients should understand the purpose of the evaluation, what information will be collected, how it will be used, and their right to refuse. In the US, requirements vary by state, and involuntary evaluations require documentation of the specific legal basis. In the UK, the Mental Capacity Act 2005 governs consent for adults, and Gillick competence applies to minors. Formal written consent is ideal; documenting verbal consent in the evaluation note is the minimum acceptable standard.
Yes. Psychiatric evaluation templates work well for telehealth sessions with some adaptations. Digital templates integrated with telehealth platforms enable real-time documentation during video sessions. Patients can complete intake forms electronically before appointments through secure patient portals. Mental status examination components adapt for virtual settings, though note that some observations (e.g. gait, psychomotor features) may be limited. Ensure your telehealth platform meets HIPAA (US) or UK GDPR compliance standards.
A psychiatric evaluation covers several broad areas through structured and open-ended questions. Clinicians ask about current symptoms (what brought you in today, how long symptoms have lasted, what makes them better or worse), psychiatric history (previous diagnoses, hospitalisations, medication trials), medical history (current conditions, medications, allergies), family history (mental health conditions in relatives), substance use (alcohol, drugs, tobacco), social history (relationships, work, housing, trauma), and current mental state (mood, sleep, appetite, thoughts of self-harm). The specific questions depend on the patient’s presenting concerns and the clinician’s assessment needs.
A psychiatric evaluation report follows a structured format that documents each assessment component in sequence. Begin with patient demographics and the reason for referral, then document the history of present illness as a chronological narrative. Record past psychiatric and medical history, family history, substance use, and social history. Include the mental status examination findings as observed during the interview. Present your diagnostic formulation with DSM-5-TR or ICD-11 codes and supporting clinical reasoning. Conclude with a treatment plan including medication recommendations, therapy referrals, safety planning if indicated, and follow-up schedule. Use clear, objective clinical language and distinguish between patient-reported information and your clinical observations.
A mental status examination (MSE) is one component within a broader psychiatric evaluation. The MSE is a structured clinical observation of the patient’s current psychological state at the time of the interview, covering appearance, behaviour, speech, mood, affect, thought process, thought content, cognition, insight, and judgment. A full psychiatric evaluation includes the MSE but also encompasses a comprehensive history (present illness, past psychiatric and medical history, family history, social history, substance use), risk assessment, diagnostic formulation, and treatment planning. Think of the MSE as a snapshot of “right now”, while the full evaluation provides the complete clinical picture.